What on Earth Does “Shape Innovation” Mean?
In brief — “Shape Innovation” stresses how implant macro- and micro-geometry guides bone healing. Aggressive threads in direct contact create primary stability, while deep grooves promote distance osteogenesis, combining the best of both regenerative mechanisms.
Sintesi (IT) — La “Shape Innovation” enfatizza come la macro- e micro-geometria implantare guidi la guarigione ossea. Spire aggressive in contatto diretto creano stabilità primaria, mentre solchi profondi favoriscono l’osteogenesi a distanza, combinando il meglio dei due meccanismi rigenerativi.
The myth of the rough surface
For years — too many years, perhaps decades — we made too much of the fact that rough-surface implants are harder to treat once peri-implantitis sets in.
That much is undeniably true. But not every implant develops the problem, thankfully. And when it does, there is usually something wrong from the start.
Those somethings have always been the same short list:
- Incorrect three-dimensional positioning (implants too close to one another, or with an emergence tilted too far to the buccal).
- Insufficient keratinized mucosa, below the canonical 2 mm.
- Prosthetic problems: crowns invading the biological width, cement left in the sulcus.
- Occlusal interferences.
- Muscle pull from frenula.
The last factor can actually shift over time, because facial and masticatory muscles remodel and often creep up toward the crest of the ridge. When the muscle insertion moves, the band of keratinized mucosa shrinks with it.
On that last point the recent literature is blunt. A meta-analysis of 30 studies (Zhang and colleagues, BMC Oral Health 2025) put numbers on what many of us had been seeing chairside for years: implants with at least 2 mm of keratinized mucosa show less plaque, less inflammation and less marginal bone loss. Roughness in itself does not condemn the implant. The biological context around it does — the tissue that receives it, the position, the occlusion. The rough surface is a convenient scapegoat.
There is also a paradox worth naming. Micrometric roughness, introduced almost thirty years ago, revolutionised osseointegration precisely because it works: as a review from Ogawa’s group at UCLA reminds us (Komatsu and colleagues, International Journal of Implant Dentistry 2024), a rough surface pushes the osteoblast to differentiate faster. But — and this is the part we tend to forget — the same roughness slows its adhesion and proliferation. A “dichotomy kinetics”, they call it. The surface, on its own, is never enough. You need the shape.
Shape guides healing
But let’s get back to “Shape Innovation”.
It is the tagline of Kalodon implants, and it is meant to bring attention back to the importance of implant micro- and macro-geometry. Surface engineering is increasingly leaning on sandblasting and acid etching to enlarge the contact area, while the once-notorious machined (smooth) surfaces are now barely represented in the implant landscape.
Shape will guide healing. Micro-geometries favour wettability in the first moments after insertion and modulate the vascularisation of the site. Macro-geometries (threads, grooves and the rest) guide bone growth from the osteotomy toward the titanium surface.
That shape matters more than we like to admit is confirmed by a review from Heimes and colleagues (International Journal of Implant Dentistry 2023): a larger diameter, a conical body and the thread profile increase the contact area with bone and, with it, primary stability — the very prerequisite of osseointegration and of any immediate-loading protocol. With one caveat I rather like, because it tempers the race toward “as long as possible”: beyond 12 mm the relationship between length and stability fades. It is not the amount of titanium that makes integration. It is the geometry.
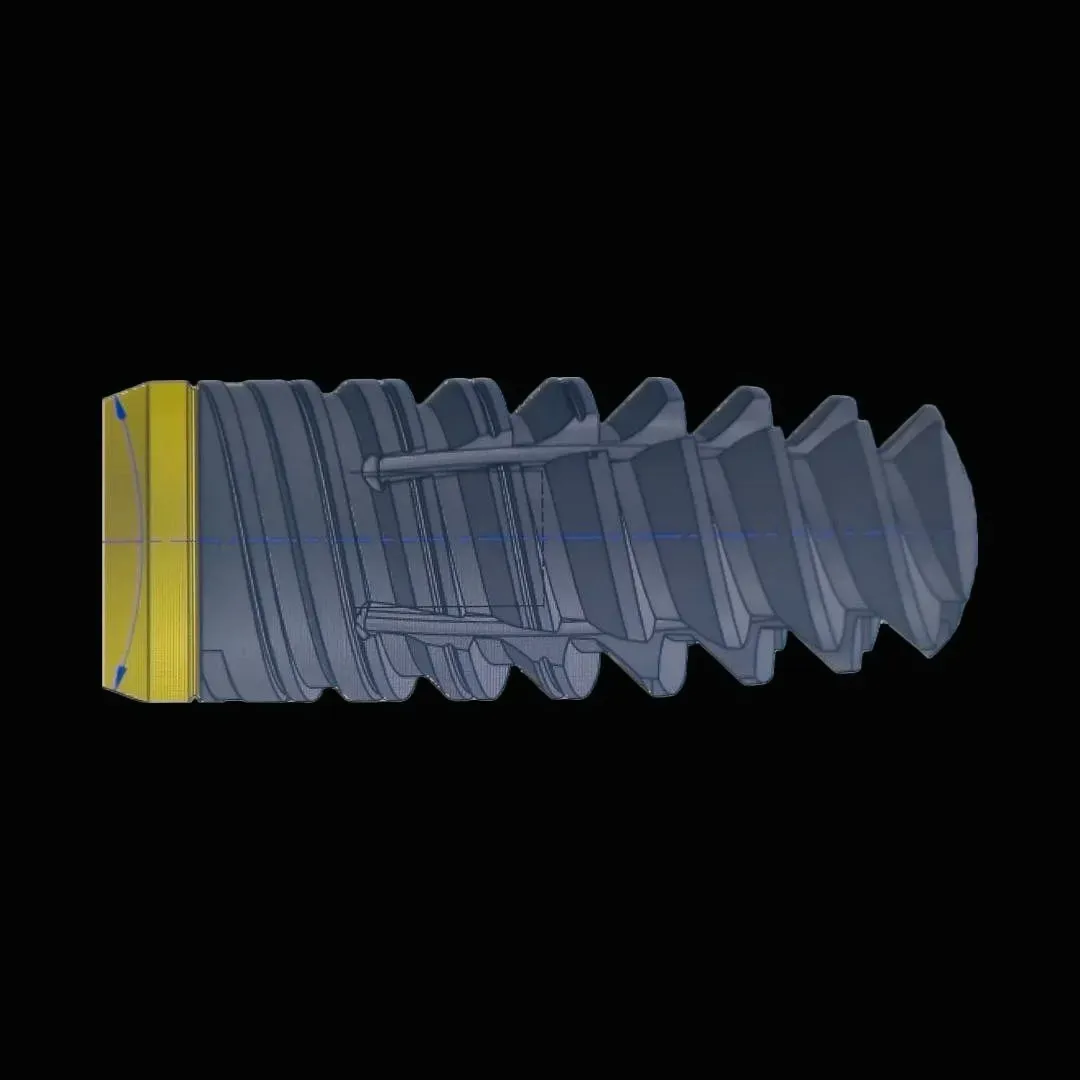
Kalodon implants — the Newton and Zerocompromise in particular — aim to guide bone healing with a deft interplay of bone contact and “non-contact”. The aggressive threads sit in direct contact with the osteotomy and forge a strong bond for primary stability, while the non-contact zones — the double-helix grooves (like DNA) that deepen toward the core of the fixture — promote the distance osteogenesis described by Davies at the University of Toronto. The right balance between distance and contact osteogenesis yields great initial stability, which allows immediate loading, and at the same time rapid ossification of the initially empty zones that prevent the implant from slipping during prosthetic manoeuvres — as so often happens with implants that are too “smooth”.
Some say distance osteogenesis does not exist (and then try to copy expansion techniques, claiming them as their own!). Others say God does not exist (fair enough, if they are agnostics). Others still try to prove the earth is flat.
But everyone must be free to express their own ideas.
“I disapprove of what you say, but I will defend to the death your right to say it.”
Evelyn Beatrice Hall
Clot chambers and regenerative implantology
Our view is that distance osteogenesis — favoured by the pits and deep grooves that cross the aggressive double threads, and that a dear friend calls “clot chambers” (because that is what they are) — is a fundamental aid in modern implantology, and even more so in regenerative implantology.
And here research has caught up with us. A preclinical study in a sheep model from Coelho’s group (Iglesias and colleagues, Biomimetics 2025) compared a traditional thread design with one featuring cutting flutes along the whole body of the implant: precisely those healing chambers we keep talking about. The result, in type IV bone — the worst, the softest — leaves little room for interpretation. The flutes distributed autologous bone chips inside the chambers, bone-to-implant contact at three weeks was significantly higher, and lateral load capacity grew by roughly two thirds. Clot chambers, in short, are not a designer’s conceit. They are the place where blood meets titanium and bone begins. It is the same logic that animates bone remodelling and, ultimately, Brånemark’s original discovery of osseointegration.
Frequently asked questions
What does “Shape Innovation” actually mean? It is the Kalodon tagline that puts implant macro- and micro-geometry back at the centre of bone healing. The smooth surface is not what decides success: it is the three-dimensional shape that orchestrates bone remodelling.
How real is the peri-implantitis risk of rough-surface implants? It has been overstated for decades. Peri-implantitis develops from problems present from the start: incorrect positioning, insufficient keratinized mucosa, prosthetic errors, occlusal interferences. Not from surface roughness alone.
What is the difference between contact and distance osteogenesis? Contact osteogenesis happens where the implant touches bone (aggressive threads). Distance osteogenesis happens in the “voids” created by deep grooves, where blood clots and cells colonise the site from the edges. Together they deliver fast, complete ossification.
Are deep grooves and “clot chambers” really necessary? Yes. Clot chambers favour the fibrin clot that serves as the natural biological matrix for bone regeneration. That is why designs with deep grooves show superior results in clinical practice.
References
- Davies JE. Mechanisms of endosseous integration. Int J Prosthodont. 1998;11(5):391-401. PMID: 9922731.
- Komatsu K, Matsuura T, Cheng J, Kido D, Park W, Ogawa T. Nanofeatured surfaces in dental implants: contemporary insights and impending challenges. Int J Implant Dent. 2024;10(1):34. DOI: 10.1186/s40729-024-00550-1. PMID: 38963524.
- Heimes D, Becker P, Pabst A, Smeets R, Kraus A, Hartmann A, et al. How does dental implant macrogeometry affect primary implant stability? A narrative review. Int J Implant Dent. 2023;9(1):20. DOI: 10.1186/s40729-023-00485-z. PMID: 37405709.
- Iglesias NJ, Nayak VV, Castellano A, Witek L, de Souza BM, Bergamo ETP, et al. The effect of three-dimensional stabilization thread design on biomechanical fixation and osseointegration in type IV bone. Biomimetics (Basel). 2025;10(6):395. DOI: 10.3390/biomimetics10060395. PMID: 40558364.
- Zhang Z, Zhang Z, Wang P, Zheng Y, Wang Z, Wang Z. The relationship between adequate keratinized mucosa and peri-implant disease: a systematic review and meta-analysis. BMC Oral Health. 2025;25(1):345. DOI: 10.1186/s12903-025-05680-5. PMID: 40050830.
FAQ
- What does "Shape Innovation" actually mean?
- It is the Kalodon tagline that puts implant macro- and micro-geometry back at the centre of bone healing. The smooth surface is not what decides success: it is the three-dimensional shape that orchestrates bone remodelling.
- How real is the peri-implantitis risk of rough-surface implants?
- It has been overstated for decades. Peri-implantitis develops from problems present from the start: incorrect positioning, insufficient keratinized mucosa, prosthetic errors, occlusal interferences. Not from surface roughness alone.
- What is the difference between contact and distance osteogenesis?
- Contact osteogenesis happens where the implant touches bone (aggressive threads). Distance osteogenesis happens in the "voids" created by deep grooves, where blood clots and cells colonise the site from the edges. Together they deliver fast, complete ossification.
- Are deep grooves and "clot chambers" really necessary?
- Yes. Clot chambers favour the fibrin clot that serves as the natural biological matrix for bone regeneration. That is why designs with deep grooves show superior results in clinical practice.
References
Looking for a specialist?
Chirurgia Orale a Frosinone →Espansione di cresta, rialzo del seno mascellare, estrazioni complesse
Need a professional opinion?
Book an appointment at Dr. Bruschi's practice in Frosinone. First visit includes full diagnosis and personalised treatment plan.
Stai valutando un impianto dentale?
Ho scritto una guida in 8 capitoli che spiega tutto quello che un paziente dovrebbe sapere prima di sedersi in poltrona. Niente marketing — solo fatti, casi studio e una checklist per fare le domande giuste.
Scarica la guidaStay Updated
New articles on periodontology, implantology and oral surgery — delivered to your inbox.
Comments
Loading comments...
Leave a comment