Help! I'm Manola and I have periodontitis

In brief — Manola’s story shows that periodontitis needs more than a clean technique: it needs honest, empathetic communication between clinician and patient. Root planing is the essential first step, and often an insufficient one; periodic reassessment decides whether regenerative surgery is needed. The mechanical removal of biofilm is what truly counts — a 2024 Cochrane review confirms that fashionable adjuncts add little. And continuity of care and trust turn out to be decisive prognostic factors.
Sintesi (IT) — La storia di Manola mostra che la parodontite richiede più di una tecnica pulita: serve una comunicazione onesta ed empatica tra clinico e paziente. La levigatura radicolare è il primo passo essenziale, e spesso insufficiente; la rivalutazione periodica decide se serve la chirurgia rigenerativa. A contare davvero è la rimozione meccanica del biofilm — una revisione Cochrane del 2024 conferma che i coadiuvanti di moda aggiungono poco. E continuità di cura e fiducia si rivelano fattori prognostici decisivi.
As dentists, some people touch us deeply with the way they face their dental problems. Every story can hand us a small lesson, a reason to reflect, a way to meet the next challenge with a little more awareness and empathy.
Provided, of course, that we can recognise our own mistakes. Because from those same mistakes you can always learn something — how to avoid, or at least handle better, the next time a similar situation comes around.
When we first met
She is a bright, lively young woman — and, underneath, very respectful and shy. Either way, her presence brings cheer.
She is one of those people who give you all of their attention. She looks you in the eye. She listens to your words. During visits, she forgets entirely that a mobile phone exists.
That way of being, on its own, commands empathy and respect.

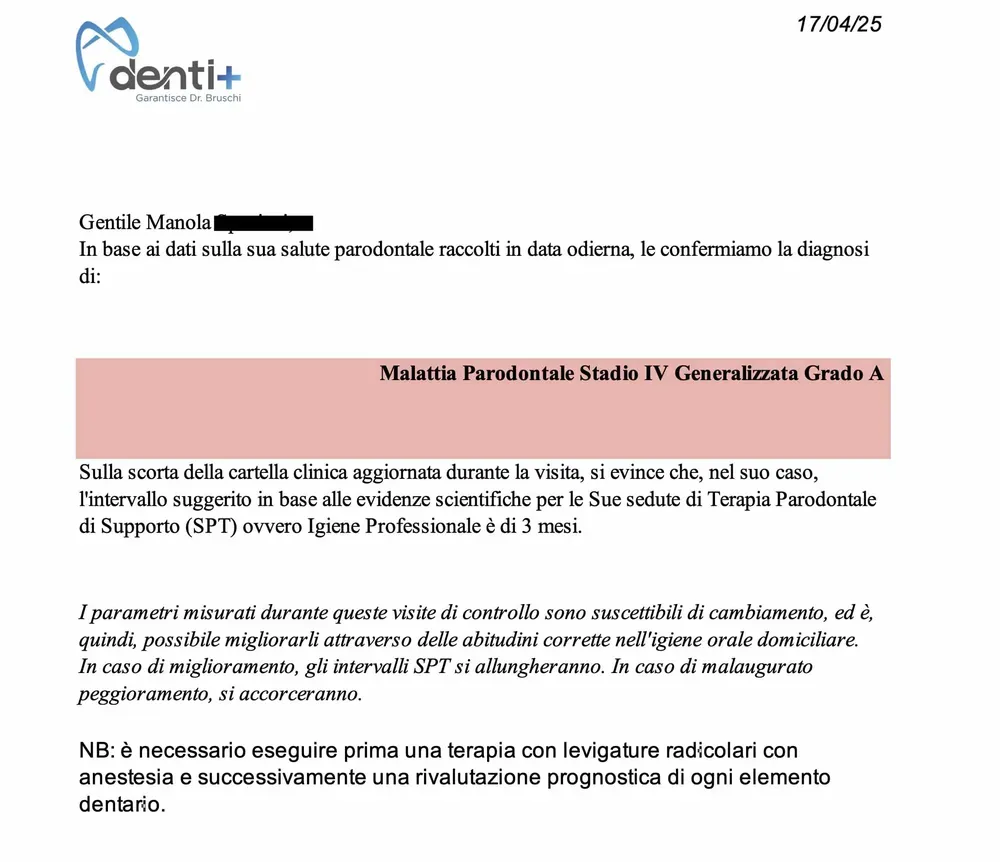
When I handed her the diagnostic certificate (which we produce for every patient with periodontal disease — see image below), Manola understood she had a serious dental problem. She is not a dentist, of course, but before I could explain the situation in plain words, her face went pale and a wave of anxiety washed over her.
The anxiety was palpable.
She could easily picture how unpleasant the consequences might be if she kept postponing — something she had been doing for a long time, while being, at least in part, aware of it. She realised that, on top of the pain and discomfort she already felt, there was a concrete risk of losing teeth, and that a long, complex course of treatment would be needed to restore her smile and her function.
How do you approach cases like this?
I proposed a first treatment with root planing under local anaesthesia and specific antibiotic prophylaxis, possibly followed by regenerative surgery for the worst sites.
Root planing was classically done with curettes — hand instruments. Today these can be paired with other tools, including ultrasonic tips and air-polishing. Generally, you use a combination of them.
In any case the next steps, as I explained to Manola, would be decided at a later reassessment appointment, some time after the root planing.
Why not decide everything right away?
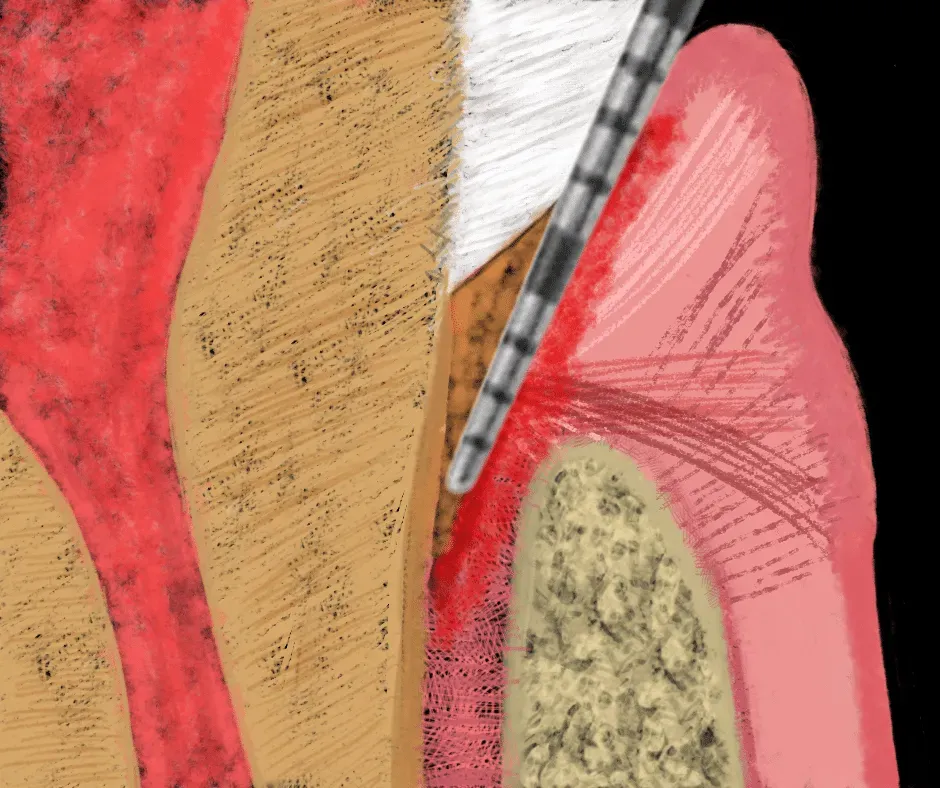
Periodontal disease — the infection caused by a biofilm loaded with periodontal pathogens — destroys the supporting tissues of the teeth. It all happens through an interplay between the bacteria, their toxins, and a body trying to defend itself.
Not all bacteria weigh the same. Some, like Porphyromonas gingivalis, even manage to invade the cells of the gum tissue and hide from the immune system. Others, like Aggregatibacter actinomycetemcomitans, are linked to the most aggressive forms — the ones that run fast in young patients. Knowing who you are dealing with changes the prognosis.
The competition takes place along the roots of the teeth and the surrounding tissue. In particular, the alveolar bone softens and is replaced by reactive granulation tissue.
We dentists usually read this inflammatory tissue as part of the reduction of the alveolar bone structure.
Yes, it is true that this infectious/inflammatory process damages the bony structure and undermines the stability of the teeth. But we must always keep in mind that, with root planing, a variable amount of mineralised tissue can be recovered.
The silent disease
As the infection advances and the granulation tissue develops, symptoms such as swelling and pain may appear; more often, though, the disease is barely symptomatic or not symptomatic at all, and the patient notices nothing.
In this light, the logic of intervening first with decontamination (root planing) rests on the fact that this — even if possibly incomplete in the deeper, less accessible zones — will lower the level of inflammation.
As mentioned in the previous section, lowering the level of inflammation, with the reduction of the molecules involved, will convert a share of reactive granulation tissue back into mineralised tissue. The bone cells are still present, even in the demineralised zone. Others appear as part of the healing process.
In essence, the alveolar bone begins to regenerate with the very first treatments.
But can root planing alone be enough to treat this disease?
In a word, yes. The sophisticated name for this treatment is non-surgical periodontal therapy. But it is a misleading name: it is performed under anaesthesia, and it is far more than a periodic hygiene recall.
And here I want to be honest, because over the years I have watched plenty of fashions come and go. Lasers, antibiotic gels, photodynamic therapy: each season brings its promise to outdo the old, laborious root planing. The Cochrane review by Jervøe-Storm and colleagues (2024), which lined up 50 controlled trials, is blunt on this point: adding photodynamic therapy to subgingival instrumentation produces no clinically meaningful improvement. What truly counts, in short, is the mechanical removal of the biofilm. Everything else is garnish. A 2025 network meta-analysis (Lin et al.) on the most severe cases — Stage III/IV Grade C — plays the same tune: adjuncts give real but small benefits, and never replace the instrument in the hygienist’s hand.
It is also worth knowing that root planing is more often insufficient. In the most severe cases, the depth of the lesions, combined with the complexity of the root anatomy, makes complete decontamination impossible without exposing the roots directly (as you do in surgery). I have written about that path in how severe periodontitis is treated.
How do you know when root planing was not enough?
You have to reassess the patient, tooth by tooth, at least with periodontal probing and new radiographs.
With the probing method, the dentist measures the depth of the gingival sulcus, which becomes a “periodontal pocket” wherever the disease persists. If the pocket bleeds, a serious infection remains. With the probe, gingival recessions are measured too.
With the radiographs, the dentist compares the before and after, and judges where the treatment was effective and sufficient and where, if needed, a different approach is required.
Where a deep bony defect remains — those vertical craters that planing alone will not fill — the chapter of guided periodontal regeneration opens. Here the long-term data are encouraging and, at the same time, a reminder to stay humble. The meta-analysis by Wang and colleagues (Periodontology 2000, 2025), which followed patients from 5 up to 20 years, shows that regenerative techniques produce a stable clinical attachment gain of around 3.3 mm and a pocket reduction of roughly 4 mm. But — and it is the “but” that matters — they do not demonstrate a clear superiority over a simple access flap. Biology, not the material, does most of the work. Autologous platelet concentrates (PRF), studied by Miron and colleagues (Periodontology 2000, 2024), add something when combined with a graft, but remain an accelerator, not a miracle.
The verdict
In Manola’s case, root planing — thanks also to the patient’s commitment and the hygienist’s skill — was very effective. Together with the hygienist we decided to keep monitoring the situation with periodic recalls. We would step in, if necessary, for site-specific problems.
The misunderstanding and the drift
Months passed, and Manola came regularly to her professional hygiene sessions with the hygienist. The clinical picture was stable. Comparing notes with the hygienist, we decided to carry on like this and then, eventually, reassess a few situations — among them some edentulous areas.
But I had not considered that Manola no longer felt she was at the centre of my attention as her dentist. From her point of view, she felt abandoned.
Mea culpa! I had made a glaring mistake, because I had not told her frankly what my intentions and my ideas about her case were.
I keep getting it wrong
One day I made another mistake, the one that made an already full glass overflow. It was a clinically intense day. I saw her at the front desk but, taken up by a hundred things, I greeted her quickly and, rather than stopping to talk, turned to the next patient on my schedule.
I was running slightly late, but even a brief conversation might have loosened a knot already pulled too tight.
The result was an argument and a withdrawal on both sides — partly because of my pride, too. I should have set it aside and tried to understand her point of view.
The interruption of care
Manola decided to turn to other colleagues to continue her treatment.
She collected her clinical chart and her radiographs.
Months passed, many months. I only had vague news of her condition. I knew she was being treated elsewhere and, honestly, I hoped she was doing well.
Yet somehow, in the workings of the new practice she was attending — probably only in Manola’s case — the right coordination between dentist and dental hygienist went missing.
It is also true that they took on a case already mid-treatment, without knowing the history well.
In the following months, Manola notices that something is wrong. She gradually worsens and suffers recurrent gum abscesses, with pain and mobility.
Confused, she feels abandoned and misunderstood once again. She turns to other periodontists, each of whom offers their own personal opinion of Manola’s disease.
As always, a fan of possibilities opens up — one that springs from each dentist’s foundational knowledge and from their clinical and surgical skills. Who would ever propose a treatment outside the range of their own technical abilities?
And just as well!
Coming back
Manola’s husband writes to me.
He tells me about his wife’s various ordeals and doubts.
I apologise, and we come back together.
She explains that she is not convinced by the treatments she has been offered. I tell her that, on the whole, they seem correct to me — except for a few.
She tells me she would like to start the journey with us again, and I accept.
With my team, we try to pick up where we left off. Unfortunately, some sites had worsened a great deal (probably also because the phase of uncertainty, without maintenance, had lasted a long time) and it was necessary to step in several times with deep root planing.
Right now, we have recovered what was possible and we will plan single implants to replace a few teeth.

Do you have questions or curiosities about this treatment, or other topics on my blog? Get in touch.
Frequently asked questions
What is periodontitis and how does it show up clinically?
Periodontitis is a bacterial biofilm infection that destroys the supporting tissues of the teeth. It often advances silently, with no obvious symptoms, until bleeding, swelling, tooth mobility or recurrent gum abscesses appear.
Why does root planing not always cure periodontitis?
Root planing decontaminates the root surfaces and lowers inflammation, allowing partial bone regeneration. But in severe cases, with deep pockets and complex root anatomy, decontamination is incomplete and later regenerative surgery or extraction may be needed.
How do you tell whether root planing worked?
Reassessment is done after 4–6 weeks with periodontal probing (pocket depth), bleeding assessment, before/after radiographic comparison and mobility testing, to identify the sites that still need further treatment.
What are the most common clinical mistakes in treating periodontitis?
Failing to communicate the treatment plan, no scheduled follow-ups, discontinuity of care between different specialists, underestimating patient compliance, and isolating the clinician from the patient’s psychosocial life all compromise the result.
References
- Jervøe-Storm PM, Bunke J, Worthington HV, Needleman I, Cosgarea R, MacDonald L, et al. Adjunctive antimicrobial photodynamic therapy for treating periodontal and peri-implant diseases. Cochrane Database Syst Rev. 2024;7(7):CD011778. doi:10.1002/14651858.CD011778.pub2. PMID: 38994711.
- Lin SY, Lin HY, Sun JS, Chang JZ. Efficacy of adjunctive periodontal interventions in non-surgical periodontal therapy for Stage III/IV Grade C periodontitis: a systematic review and network meta-analysis. Jpn Dent Sci Rev. 2025;61:167-187. doi:10.1016/j.jdsr.2025.07.001. PMID: 40697931.
- Wang HL, Hazrati P, Calatrava J, Saleh MS, Alrmali AE. Long-term clinical outcomes of periodontal regeneration of intrabony defects: a systematic review and meta-analysis. Periodontol 2000. 2025. doi:10.1111/prd.70002. PMID: 40931709.
- Miron RJ, Moraschini V, Estrin N, Shibli JA, Cosgarea R, Jepsen K, et al. Autogenous platelet concentrates for treatment of intrabony defects — a systematic review with meta-analysis. Periodontol 2000. 2024;97(1):153-190. doi:10.1111/prd.12598. PMID: 39425513.
- Forshaw R. Dental calculus — oral health, forensic studies and archaeology: a review. Br Dent J. 2022;233(11):961-967. doi:10.1038/s41415-022-5266-7. PMID: 36494546.
Evidence source: PubMed.
FAQ
- What is periodontitis and how does it show up clinically?
- Periodontitis is a bacterial biofilm infection that destroys the supporting tissues of the teeth. It often advances silently, with no obvious symptoms, until bleeding, swelling, tooth mobility or recurrent gum abscesses appear.
- Why does root planing not always cure periodontitis?
- Root planing decontaminates the root surfaces and lowers inflammation, allowing partial bone regeneration. But in severe cases, with deep pockets and complex root anatomy, decontamination is incomplete and later regenerative surgery or extraction may be needed.
- How do you tell whether root planing worked?
- Reassessment is done after 4–6 weeks with periodontal probing (pocket depth), bleeding assessment, before/after radiographic comparison and mobility testing, to identify the sites that still need further treatment.
- What are the most common clinical mistakes in treating periodontitis?
- Failing to communicate the treatment plan, no scheduled follow-ups, discontinuity of care between different specialists, underestimating patient compliance, and isolating the clinician from the patient's psychosocial life all compromise the result.
References
Looking for a specialist?
Innesto Osseo a Frosinone →Tipi di innesto, tecniche e indicazioni per ricostruire l'osso perduto
Need a professional opinion?
Book an appointment at Dr. Bruschi's practice in Frosinone. First visit includes full diagnosis and personalised treatment plan.
Stai valutando un impianto dentale?
Ho scritto una guida in 8 capitoli che spiega tutto quello che un paziente dovrebbe sapere prima di sedersi in poltrona. Niente marketing — solo fatti, casi studio e una checklist per fare le domande giuste.
Scarica la guidaStay Updated
New articles on periodontology, implantology and oral surgery — delivered to your inbox.
Comments
Loading comments...
Leave a comment