A Friend's Story: Rebuilding an Implant-Supported Prosthesis That No Longer Holds

In brief — The story of a patient with falsely seated implants placed in the wrong position and terminal periodontal disease. By removing the incongruous implants, placing new ones, and regenerating the mucosa without connective tissue xenografts, complete alveolar anatomy was restored — and so was the patient’s vitality.
Sintesi (IT) — La storia di un paziente con impianti malposizionati e malattia parodontale terminale. Rimuovendo gli impianti incongrui, inserendone di nuovi e rigenerando la mucosa senza xenoinnesti di connettivo, è stata ottenuta la completa rigenerazione dell’anatomia alveolare e la rinascita della vitalità del paziente.
The mouth is life
When do we become old?
There are many reasons. Surely one of them is no longer being able to use your mouth to eat efficiently and without pain. And it isn’t only about eating: with the mouth we speak and relate to others, we go out to dinner feeling at ease, we smile back at someone’s smile, we laugh at a joke or a comedy and — not least — through the mouth passes our affection. With the mouth we kiss those we love and our partner. The mouth carries a strong erotic charge: why not?!
If the mouth is not in order, all of this is lost. And more often than not, this happens as the years go by.
Back to my friend. He had a problem. He was a dynamic, vital man. Then, at a certain point, his heart gave out. And what did he do? Did he give up? On the contrary, he had himself treated and went back to being even more active, taking up competitive sport. Time proved him right: he doesn’t look his age at all — he seems decidedly younger, with a physique and a vitality the young might envy.
But one problem remained. My friend had a devastated mouth. He already had implants, but they no longer held.
Diagnosis and treatment plan
When I examined him, I realised that some implants were still osteointegrated, but the connection between implants and the prosthesis above them was ruined beyond repair.
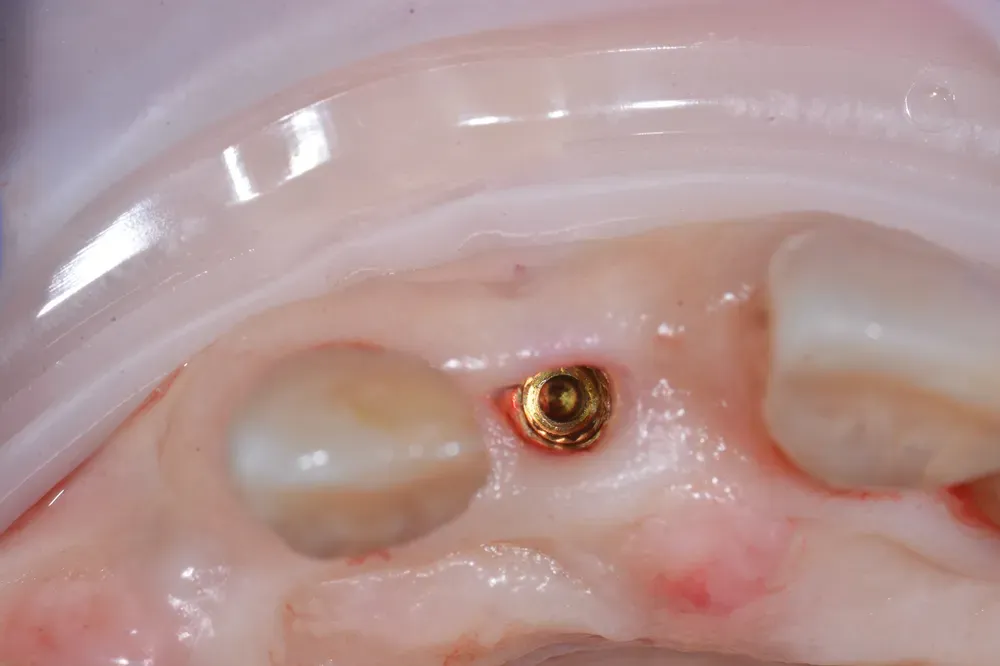
Other implants had been placed incorrectly and were about to fail for lack of congruent bone walls (see the figure below).
On top of that, many teeth had already been lost to periodontal disease, which — incidentally — posed serious risks for his delicate cardiac situation. When such teeth cannot be effectively treated, it is preferable to replace them with implants.
Let me pause on a question many colleagues ask me: isn’t removing malpositioned implants and placing new ones in the same surgical session a gamble? Recent evidence says no — provided you respect rigorous criteria. A systematic review with meta-analysis published in the Journal of Prosthetic Dentistry by Chen and colleagues in 2024 pooled 23 studies on 630 implants placed immediately into sockets with bone defects in the aesthetic zone: implant survival was 98.1%, with Pink Esthetic Scores of 12.3–12.6 at 12 and 24 months. Campi and colleagues, also in 2024 in Quintessence International, reached the same conclusion analysing only randomised trials on compromised sockets: 100% survival and outcomes comparable to those achieved in intact sockets. The immediate implant is therefore not a risky shortcut: it is a predictable procedure, when the diagnosis is honest and the hand is steady.
At this point we began to reason together about the possible solutions, and he gave me his trust; I thank him, because thanks to that we managed to obtain the very best for him.
I proposed removing the old implants and replacing them immediately with new ones, then moving to a provisional bridge with the extraction of the compromised teeth and the total regeneration of the anatomical form of the osteomucosal arch — so that we could finally build a bridge supported by implants, with a shape and colour resembling natural teeth. The photos that follow illustrate some phases of this work.

We removed the old implants easily and replaced them with new ones. We added others, performing heterologous bone grafts and a maxillary sinus lift, given that we would later have to extract some unmaintainable teeth.
When we removed the teeth with terminal periodontal disease, we inserted a provisional bridge supported by the new implants — an immediate-loading restoration that fitted into the sockets of the extracted teeth (ovate pontics). This is a consolidated technique for preserving the form of the arch, which (I personally) learned in Sweden from my esteemed professors Lindhe and Wennström.
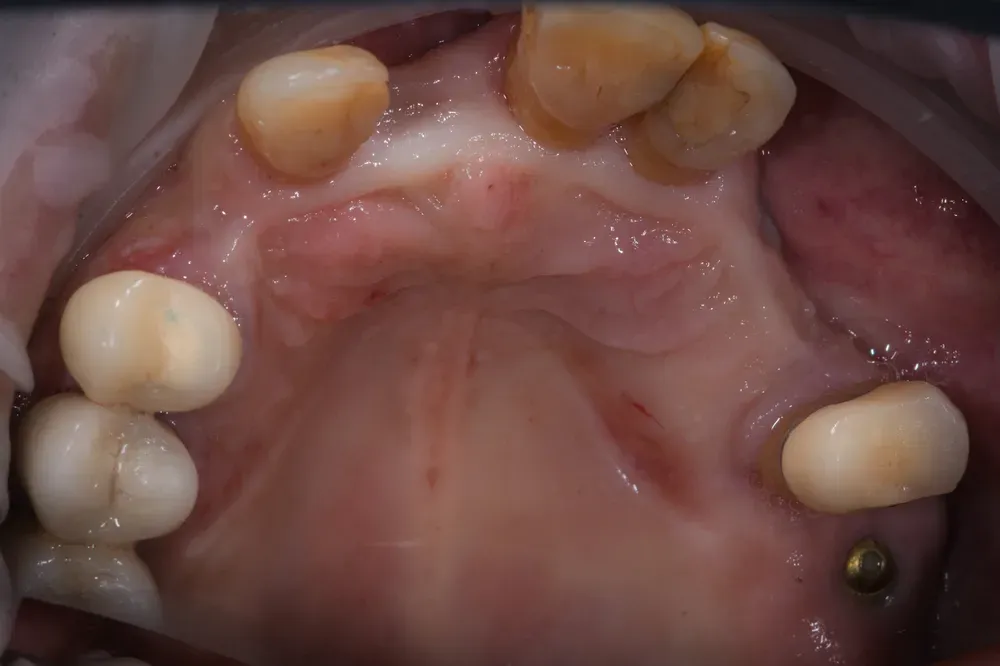
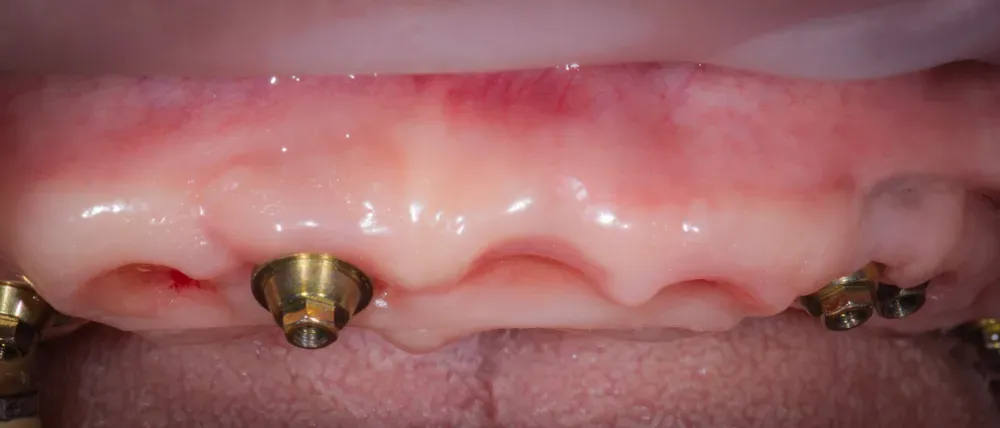
In the two figures below it is clear how the therapy — here still in the phase of extracting the unmaintainable teeth — achieves the total restoration (regeneration) of the alveolar tissue, and therefore a form entirely similar to the natural one. And this is obtained only through mucosal expansion of the site and without connective tissue xenografts. Moreover, nothing was inserted into the extraction sockets to maintain the form: the shape is held only by the profile of the provisional, which seats 4 mm inside with the “ovate pontics”.

Regeneration without biomaterials
In short, regeneration is obtained with air — or rather, with the blood that fills the voids, and then thanks to the cells that colonise the site from the edges, with no other material added. Beautiful, isn’t it?
Of course, materials are sold and air (still) is not. But it is worth knowing that this possibility exists, for every colleague and every patient who chooses to take it up.
Here I have to be precise, because the literature should be read in full and not by halves. The ovate pontic — the pontic that slips into the socket and shapes the mucosa — is neither my invention nor a niche oddity. In a prospective clinical study published in the Journal of Prosthodontics in 2025, Kim and Tarnow measured what happens around an ovate pontic placed immediately after extraction: with ridge preservation, the dimensional changes of the crest at six months stay contained (a little over a millimetre in width and height), and the natural morphology is maintained regardless of the buccal bone wall. This is exactly the principle I apply here: the shape of the provisional guides the tissue, and the blood does the rest.
And connective tissue grafts? The question is legitimate, because for decades the palatal harvest was the reference for thickening the mucosa. The truth, today, is more nuanced. A 2024 network meta-analysis in Clinical Oral Investigations (Tommasato, Sculean, Canullo and colleagues) confirms that the connective tissue graft remains the most effective material when the goal is to increase the thickness of peri-implant tissues. But when the goal is different — preserving a contour, rebuilding an anatomy with what the site already owns — adding heterologous tissue or a second surgical site stops being mandatory. Knowing when a graft is truly needed and when it is not is half the craft. This, in the end, is the same philosophy that drives bonebending versus traditional bone regeneration: less material, more biology.
How did my friend’s journey continue?
We took a scan with an intraoral scanner to finalise the work in ceramic and — thanks to the new teeth made possible by the form of the gums you see in the images below — he resumed his dynamic life, happier than before, able to fully enjoy every one of his days thanks also to his new teeth! And he deserves all of this, and more: believe me.

Frequently asked questions
When is it indicated to remove “incongruous” implants? When implants are placed in the wrong position (too buccal, too proximal) without congruent bone walls, they create a situation predisposed to failure. Removal and replacement with correct positioning is the most rational long-term path.
How is mucosal regeneration achieved without connective tissue xenografts? Through the ovate pontic technique: a provisional inserted 4mm into the extraction sockets. The mucosa expands naturally, blood fills the initial voids, and cells colonise the site from the edges with no added material. It is pure biological regeneration.
How long does full-arch regeneration take? With the protocol described (a provisional bridge with ovate pontics), regeneration of the anatomical form of mucosa and bone takes roughly 4-6 months. The definitive ceramic restoration follows once the tissues have stabilised.
What are the advantages of regeneration without biomaterials? Lower costs, no biological risk from heterologous materials, faster healing, and a natural biological process. Patients are often surprised by how regenerative nature can be when supported by the right technique.
References
- Kim SR, Song SJ, Urban J, Wu W, Bittner N, Tarnow DP. Comparison of dimensional changes and ridge contour around ovate pontics inserted immediately after extraction with and without buccal bone plate with different grafting procedures. J Prosthodont. 2025. doi:10.1111/jopr.14050 · PMID: 40135604
- Campi M, Leitão-Almeida B, Pereira M, Shibli JA, Levin L, Hasse Fernandes JC, et al. Immediate implant placement in damaged extraction sockets: a systematic review and meta-analysis of randomized controlled trials. Quintessence Int. 2025;56(1):34-45. doi:10.3290/j.qi.b5768294 · PMID: 39351790
- Chen R, Xu J, Wang S, Duan S, Wang Z, Zhang X, et al. Effectiveness of immediate implant placement into defective sockets in the esthetic zone: a systematic review and meta-analysis. J Prosthet Dent. 2024;133(2):411-426. doi:10.1016/j.prosdent.2024.02.022 · PMID: 38493065
- Tommasato G, Del Fabbro M, Oliva N, Khijmatgar S, Grusovin MG, Sculean A, et al. Autogenous graft versus collagen matrices for peri-implant soft tissue augmentation. A systematic review and network meta-analysis. Clin Oral Investig. 2024;28(5):300. doi:10.1007/s00784-024-05684-5 · PMID: 38704784
FAQ
- When is it indicated to remove "incongruous" implants?
- When implants are placed in the wrong position (too buccal, too proximal) without congruent bone walls, they create a situation predisposed to failure. Removal and replacement with correct positioning is the most rational long-term path.
- How is mucosal regeneration achieved without connective tissue xenografts?
- Through the ovate pontic technique: a provisional inserted 4mm into the extraction sockets. The mucosa expands naturally, blood fills the initial voids, and cells colonise the site from the edges with no added material. It is pure biological regeneration.
- How long does full-arch regeneration take?
- With the protocol described (a provisional bridge with ovate pontics), regeneration of the anatomical form of mucosa and bone takes roughly 4-6 months. The definitive ceramic restoration follows once the tissues have stabilised.
- What are the advantages of regeneration without biomaterials?
- Lower costs, no biological risk from heterologous materials, faster healing, and a natural biological process. Patients are often surprised by how regenerative nature can be when supported by the right technique.
References
Looking for a specialist?
Rigenerazione Ossea a Frosinone →Il Metodo Bonebenders: espansione osteo-mucosa senza innesti
Need a professional opinion?
Book an appointment at Dr. Bruschi's practice in Frosinone. First visit includes full diagnosis and personalised treatment plan.
Stai valutando un impianto dentale?
Ho scritto una guida in 8 capitoli che spiega tutto quello che un paziente dovrebbe sapere prima di sedersi in poltrona. Niente marketing — solo fatti, casi studio e una checklist per fare le domande giuste.
Scarica la guidaStay Updated
New articles on periodontology, implantology and oral surgery — delivered to your inbox.
Comments
Loading comments...
Leave a comment