Split Crest: Does the Partial-Thickness Flap Really Matter?
In brief — Split crest works only with a partial-thickness flap. Stripping the bone means tearing away the periosteum, the progenitor cells, the vascularization that keeps the mobilized cortex alive. The gap fills with new bone only if the wall stays vital. Everything else is folklore that produces failures blamed on the technique instead of on who performs it.
Sintesi (IT) — La split crest funziona solo con lembo a spessore parziale. Denudare l’osso significa strappare via il periostio, le cellule progenitrici, la vascolarizzazione che mantiene viva la corticale mobilizzata. Tutto il resto è folklore che genera fallimenti attribuiti alla tecnica invece che a chi la esegue.
The most common mistake in split crest (ERE, for us) is convincing yourself that it’s just… a split crest!
They say it doesn’t work, that it’s obsolete, unreliable, outdated.
And then I see someone do it.
And I also see how they do it.
And I put my hands in my hair.
Every regenerative technique has requirements. In GBR it’s flap passivity. In split crest/ERE it’s the partial-thickness flap.
That’s how it’s done. You can’t do it like it’s 1930 and then claim it doesn’t work.
Because it’s true. If you do it that way, the bone will melt away like snow in the sun.
And yours doesn’t resorb? That means you had the thickness and it wasn’t a split case to begin with.
If you denude a thin cortex, it will largely resorb.
The Periosteum Is Not Optional
When Bruschi (my father) and Scipioni presented their ridge expansion protocol in 1994, they didn’t name it “Edentulous Ridge Expansion” (ERE) by chance.
Why such a cryptic acronym?
We’re in the nineties, an era of pure “acronym-mania”: ASAP, LOL and the legendary MTV are emblematic acronyms of those years. You had to stand out, distinguishing yourself from “split crest”. That’s how ERE was born, an innovative procedure based on a partial-thickness flap and an approach that is decidedly more periodontist than implantologist.
So they defined it on a precise biological principle: the regenerative potential of alveolar bone works only if the periosteum is preserved.
Not as an option. Not as a technical detail for purists. As a conditio sine qua non.
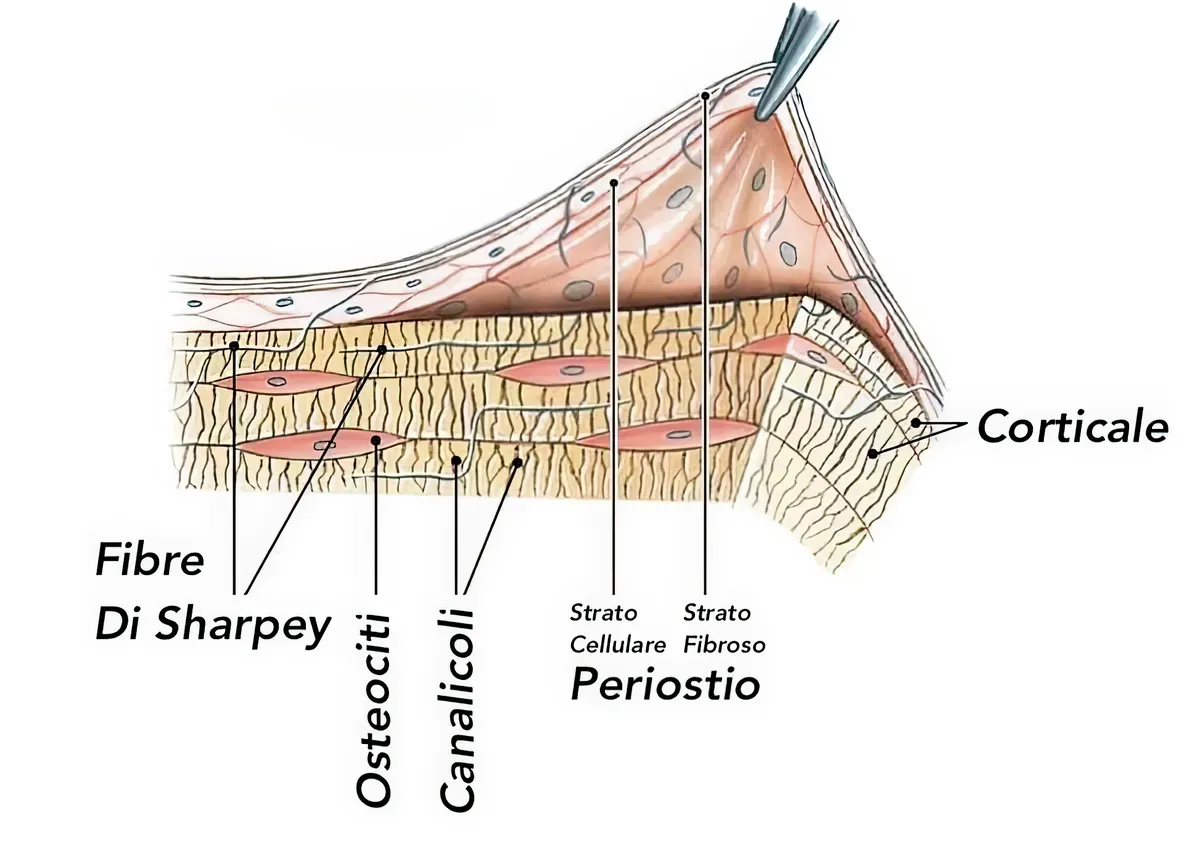
The periosteum isn’t just that adherent fibrous tissue you lift to see the underlying alveolar bone.
It’s a biological structure that holds the osteoblast progenitor cells, the vascularization that keeps the outer cortex alive, and the whole biological infrastructure that lets the gap created by the split fill with new bone instead of fibrous tissue.
And it’s also a biomechanical structure. The presence of this connective tissue makes the underlying bone wall more elastic, moldable, and fracture-resistant.
Raising a full-thickness flap means tearing away this infrastructure, like removing the irrigation system from a field before sowing.
I’m Not Saying It. The Literature Says It.
H. Staffileno et al.
Back in the 1960s and ’70s, the studies by Harry Staffileno Jr. and colleagues demonstrated, through experimental histologic research, the superiority of the partial-thickness flap over the traditional mucoperiosteal flap for preserving alveolar bone in periodontal surgery.
The split-thickness technique, which involves an incision through epithelium and connective tissue while leaving the periosteum intact on the bone, produces significantly less bone resorption than the full-thickness flap.
Histologic investigations revealed that in the mucoperiosteal flap the resorption involves the entire layer of circumferential lamellae and portions of the underlying Haversian systems, whereas with the partial-thickness flap the osteoclastic activity is limited to a few superficial reversal lines without affecting the Haversian systems.
Moreover, the healing process is accelerated by a few days, with the interface between the flap’s connective tissue and the periosteal connective tissue allowing faster repair than the bone-to-soft-tissue interface of the full-thickness flap.
The original papers can be found at the following links:
- Staffileno H, Levy S, Gargiulo A. Histologic study of cellular mobilization and repair following a periosteal retention operation via split thickness mucogingival flap surgery. J Periodontol. 1966 Mar-Apr;37(2):117-31. PMID: 5217762.
- Staffileno H Jr. Palatal flap surgery: mucosal flap (split thickness) and its advantages over the mucoperiosteal flap. J Periodontol. 1969 Sep;40(9):547-52. PMID: 5259738.
- Staffileno H. Significant differences and advantages between the full thickness and split thickness flaps. J Periodontol. 1974 Jun;45(6):421-5. PMID: 4525958.
The differences between partial-thickness and full-thickness periodontal surgery (according to the cited studies) are summarized in the following table:
| Parameter | Full-thickness flap (mucoperiosteal) | Partial-thickness flap (split thickness / mucosal) | Main reference (year) |
|---|---|---|---|
| Technical definition | Incision and elevation including epithelium, connective tissue and periosteum down to the bone (bone fully exposed). | Incision and dissection of epithelium and part of the connective tissue, leaving the periosteum adherent to the bone. | 1974; 1969; 1966 |
| Periosteum | Removed and reflected with the flap. | Preserved, maintains vascular and cellular continuity. | 1966; 1974 |
| Flap vascularization | Partly compromised by loss of periosteal supply. | Maintained, double supply (from the connective tissue and the underlying periosteum). | 1969; 1974 |
| Surgical trauma | Greater: bone exposure and superficial bone necrosis. | Lower: no direct bone exposure. | 1969; 1974 |
| Osteoclastic activity (bone resorption) | High: involves circumferential lamellae and Haversian systems; crestal margin resorption. | Limited and superficial; stops within 14 days; crest preserved. | 1966; 1974 |
| Osteogenesis / bone reconstruction | Delayed; starts after 21 days, incomplete at 60 days. | Early (already at 14–21 days); complete restitutio ad integrum at 60 days. | 1966; 1974 |
| Post-surgical alveolar anatomy | Deformed: crestal resorption and attachment recession. | Preserved: no anatomical deformity; stable attachment. | 1966; 1974 |
| Post-op pain and bleeding | Greater; risk of extravasation from periosteal loss. | Lower; easier hemostasis and more comfortable recovery. | 1969 |
| Overall healing time | Slower (a few days behind the partial-thickness flap). | Faster and biologically more predictable. | 1974 |
| Synthesis | More traumatic procedure, with greater resorption and long healing times; reserve for selected cases. | Biologically superior: preserves bone, periosteum and gingival architecture; indicated in most mucogingival surgery. | 1966–1974 (synthesis) |
It’s worth remembering that Staffileno was a highly respected and well-known figure. Among his many roles and academic appointments, he also served as president of the AAP.
Ole T. Jensen
Ole Jensen needs no introduction, and he’s someone who understands jaw expansion. He comes from the school of William Harrison Bell, the maxillofacial surgeon who fathered the Le Fort I osteotomy and a great revolutionary of orthognathic surgery.
I recommend everyone keep a fundamental Jensen text in their library, one about jaw expansion techniques:
“Osteoperiosteal Flap” is a suggestive and, at the same time, very concrete title. It underscores how the integrity of the periosteum is essential to preserve the plasticity of the system and to allow the expansive maneuvers.
Jensen and colleagues published in 2009 in the Journal of Oral and Maxillofacial Surgery a comparative study that should be printed and framed in every operating room where implant dentistry is practiced.
They compared three flap approaches in the split crest (ERE): full-thickness flap, partial-thickness flap, and minimal osteoperiosteal (almost flapless) flap. The one-year results leave no room for interpretation:
Most of the cases treated with a full-thickness flap showed buccal bone loss and gingival recession.
The partial-thickness and minimal osteoperiosteal flaps showed stable bone patterns.
The study’s conclusion is that full-thickness mucoperiosteal flaps should not be reflected when performing a split crest.
Not “might not be the best choice”. Not “should be evaluated case by case”. Should not be reflected. Full stop.
Stefan Fickl’s research from Würzburg
The histologic research by Fickl and colleagues, published in the Journal of Clinical Periodontology in 2011, evaluated bone alterations in five beagles, comparing partial- and full-thickness flaps:
Fickl S, Kebschull M, Schupbach P, Zuhr O, Schlagenhauf U, Hürzeler MB. Bone loss after full-thickness and partial-thickness flap elevation. J Clin Periodontol 2011; 38: 157–162. doi: 10.1111/j.1600-051X.2010.01658.x
After four months, elevating either type of flap resulted in bone loss and high osteoclastic activity, but the partial-thickness flaps generally showed less bone loss than the full-thickness flaps.
For intellectual honesty, I’ll point out that this paper doesn’t give definitive answers. But looking at the surgical images, I have several questions about the technique.
After all, a partial-thickness flap made with a 15c blade is an oxymoron.
Mounir et al. (2014)
This study again compares the two flap types in split crest surgery with immediate implant placement in the anterior maxilla:
Mounir M, Beheiri G, El-Beialy W. Assessment of marginal bone loss using full thickness versus partial thickness flaps for alveolar ridge splitting and immediate implant placement in the anterior maxilla. Int J Oral Maxillofac Surg. 2014;43(11):1373-80. doi: 10.1016/j.ijom.2014.05.021
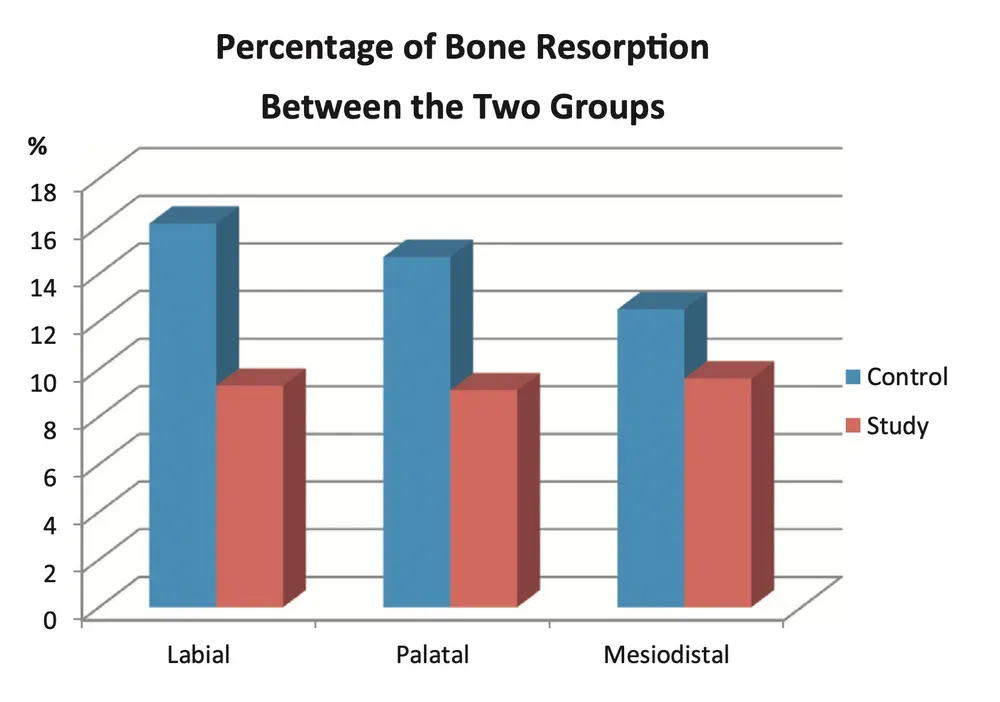
In the control group the authors used a full-thickness mucoperiosteal flap; in the study group, a partial-thickness flap. They placed 43 implants and measured marginal bone loss with CBCT at six months.
Result: the partial-thickness flap significantly reduces bone loss compared with the full-thickness flap: 9.5% less for the buccal cortex, 7.9% for the palatal, 3.5% for the mesiodistal.
The recent meta-analyses line up the numbers
So much for the history and the individual studies. But what does the most up-to-date quantitative synthesis say? Over the last two years, three meta-analyses have lined up the data, and the data don’t leave much room for opinion.
Al Haydar and colleagues (Int J Oral Maxillofac Implants, 2023) pooled 35 studies: mean horizontal gain of 3.06 mm and an implant survival rate of 98.17% across 4,446 implants. One detail worth reading twice: the gain did not change whether or not graft material was placed in the gap. It’s the living mobilized wall that does the work, not the filler. Lin and colleagues (BMC Oral Health, 2023), across 25 studies, land almost in the same spot: 3.35 mm of gain and 98.1% survival. Azadi and colleagues (Oral Maxillofac Surg, 2025), narrowing the field to graftless expansion with simultaneous implant placement, report 100% short-term survival.
Numbers any regenerative technique would sign off on immediately. But they’re averages. And inside an average, the easy cases that work anyway sit right next to the hard cases that forgive only correct execution. The meta-analysis won’t tell you which half of the distribution your next case falls into. The flap you choose will.
And then there’s the study that, in my view, should close the debate. Alotaibi and colleagues (Clin Oral Implants Res, 2025), in a network meta-analysis of randomized trials only, measured early bone resorption across vertical augmentation techniques. Verdict: the techniques that preserve the periosteum resorb less, and when a full-thickness flap is raised you must budget for volume loss at re-entry. They’re talking about vertical augmentation, not split crest. But the biological principle is the same and knows no procedural borders: take the periosteum away, and sooner or later you pay in bone.
The Illusion of Success in Easy Cases
The problem is that split crest with a full-thickness flap can work too.
Sometimes. In cases where the crest already has six or seven millimeters of thickness and you want to reach eight. In cases where the split serves more to create space for a generous-diameter implant than to solve real atrophy. In cases, in other words, where the split crest wasn’t really needed.
These are the cases that even end up in congress photos. They’re the cases that convince the colleague that his technique works. They’re the cases that create the illusion that denuding the bone is harmless. But they’re also the cases that would work with any approach, including placing the implant directly without any split at all.
The real cases, the ones with 2-4 millimeters of crest that must become 6-8, the ones with soft bone and a smoking patient, require the mobilized buccal cortex to keep its vascularization.
These cases don’t forgive. Stripped of its connective tissue, the cortex behaves like a free graft and largely resorbs.
Heat as the Coup de Grâce
But there’s worse. Many colleagues use piezoelectric inserts for the crestal osteotomy, convinced that the instrument’s precision compensates for the flap error. It compensates for nothing. It makes things worse.
I’m not saying they shouldn’t be used at all. But you need extreme caution.
Vibrating inserts generate heat. A lot of heat. Even under abundant irrigation, the local temperature easily exceeds forty degrees in the areas of greatest friction.
In normally vascularized bone this isn’t a fatal problem. Blood flow disperses the heat and buffers the thermal damage.
But in bone denuded of its periosteum, with vascularization already compromised by the elevation, that heat becomes the coup de grâce.

The bone cells that survived the denudation are cooked by the vibration. The minimal residual perfusion is wiped out. The mobilized cortex becomes a piece of devitalized bone that only waits to be resorbed.
Biology Doesn’t Negotiate
The gap created by the split fills with a clot. The clot becomes osteoid tissue at a rate of 1 μm per day. The osteoid mineralizes in ten days and becomes woven bone.
But this requires the mobilized buccal cortex to stay vital, able to receive the progenitor cells that migrate from the periosteum and from the underlying bone.
A denuded and overheated cortex can do none of this. It just sits there, inert, while the body decides what to do with it. And it will have to digest the necrotic parts before regenerating them.
What to Do Instead
The answer is simple but demands more technical attention.
The flap must be partial-thickness. You must preserve the connective tissue just above the bone (it’s not only the periosteum, of course).
The best way to do this is with round-headed blades, such as the Beaver 64 and 69. The 69 is smaller and wonderful for periodontal surgery too. The 64 can also be used for an initial bone incision in very complex cases.


The blade must separate the connective tissue in the deep layers, leaving a portion of tissue (including the thin periosteum) adherent to the cortex.
A very important instrument, which safely speeds up the split-thickness dissection at the crest and helps to build a laterally repositioned flap, is the Orban gingivectomy knife.

It’s a classic periodontal knife. Used here not for a gingivectomy but for a sophisticated flap. It must be sharpened by hand.
Why Do It This Way
Preserving the supracrestal connective tissue has countless advantages, as we’ve seen above.
It maintains the blood supply and the vitality of the cortex you’re about to mobilize. It maintains the progenitor cells. It maintains, in other words, all the biological conditions that let the split crest ERE work even in the hard cases, the ones where it truly matters.
For the osteotomy, low-speed rotary instruments (100-200) with good irrigation remain the safest choice.
If you prefer piezo for precision, irrigation must be abundant to the point of being annoying and the progression must be slow. Very slow.
But the best and least traumatic instrument remains the low-speed diamond disc.
Heat is the invisible enemy that compromises results that look mechanically perfect.
When you see that nice white bone whitening even more under the piezo, what do you think happens to it immediately afterward?
The Technique Is Not the Problem
Split crest isn’t a difficult technique.
It’s a technique that, like all regenerative ones, demands accuracy in the preparation.
Denuding the bone is a mistake. Overheating it is a mistake. Doing both is guaranteeing yourself a resorption that will then be blamed on the technique instead of the execution.
The easy cases work anyway. The hard cases, the ones where the split crest makes the difference between placing an implant and having to resort to more complex regenerations, require every step to respect biology.
Scipioni and Bruschi understood it thirty years ago.
Jensen proved it with clinical certainty fifteen years ago. Staffileno confirmed his theory histologically in the periodontium back in the 1960s.
Biology hasn’t changed in the meantime. Only our ability to ignore it has changed, while we convince ourselves that the new piezoelectric insert will solve the problem we created with the wrong flap.
Split crest works. But it works only if you do it the way it must be done. With the periosteum preserved, with instruments that don’t fry the osteoblasts, with respect for a biology that doesn’t negotiate with our technical preferences.
Everything else is folklore that produces failures blamed on the technique instead of on who performs it.
References
- Al Haydar B, Kang P, Momen-Heravi F. Efficacy of Horizontal Alveolar Ridge Expansion Through the Alveolar Ridge Split Procedure: A Systematic Review and Meta-Analysis. Int J Oral Maxillofac Implants. 2023;38(6):1083-1096. doi:10.11607/jomi.9972. PMID: 38085739.
- Lin Y, Li G, Xu T, Zhou X, Luo F. The efficacy of alveolar ridge split on implants: a systematic review and meta-analysis. BMC Oral Health. 2023;23(1):894. doi:10.1186/s12903-023-03643-2. PMID: 37986181.
- Azadi A, Hazrati P, Tizno A, Rezaei F, Akbarzadeh Baghban A, Tabrizi R. Bone expansion as a horizontal alveolar ridge augmentation technique: a systematic review and meta-analysis. Oral Maxillofac Surg. 2025;29(1):32. doi:10.1007/s10006-025-01335-5. PMID: 39808204.
- Alotaibi FF, Buti J, Rocchietta I, Mohamed Nazari NS, Almujaydil R, D’Aiuto F. Premature Bone Resorption in Vertical Ridge Augmentation: A Systematic Review and Network Meta-Analysis of Randomised Clinical Trials. Clin Oral Implants Res. 2025;36(7):787-801. doi:10.1111/clr.14435. PMID: 40116110.
- Mounir M, Beheiri G, El-Beialy W. Assessment of marginal bone loss using full thickness versus partial thickness flaps for alveolar ridge splitting and immediate implant placement in the anterior maxilla. Int J Oral Maxillofac Surg. 2014;43(11):1373-1380. doi:10.1016/j.ijom.2014.05.021. PMID: 24973295.
- Fickl S, Kebschull M, Schupbach P, Zuhr O, Schlagenhauf U, Hürzeler MB. Bone loss after full-thickness and partial-thickness flap elevation. J Clin Periodontol. 2011;38(2):157-162. doi:10.1111/j.1600-051X.2010.01658.x. PMID: 21118288.
❓ Frequently Asked Questions (FAQ)
Why is the partial-thickness flap so important in split crest?
The periosteum and the supracrestal connective tissue hold the osteoblast progenitor cells and the vascular supply that keeps the outer cortex alive. When you mobilize the buccal cortex with the split, it stays attached to the periosteum and keeps its vitality. The gap fills with a clot that turns into new bone only if the mobilized wall stays alive. Stripping the bone with a full-thickness flap tears away this biological infrastructure. A denuded cortex behaves like a free graft with no vascularization and largely resorbs.
Can I use piezosurgery for the split crest?
Piezosurgery can be used, but with extreme caution. Vibrating inserts generate a lot of heat even under abundant irrigation, easily exceeding forty degrees in the areas of greatest friction. In normally vascularized bone the blood flow disperses the heat, but in bone already denuded of its periosteum with compromised vascularization, that heat becomes lethal for the cells. If you prefer piezo for precision, irrigation must be abundant to the point of being annoying and the progression very slow. Low-speed rotary instruments (100-200 rpm) with good irrigation remain the safest choice.
Which instruments do I need to make a proper partial-thickness flap?
The ideal instruments are round-headed blades such as the Beaver 64 and 69. The Beaver 69 is smaller and excellent for periodontal surgery too. The Beaver 64 can also be used for an initial bone incision in very complex cases. These blades separate the connective tissue in the deep layers, leaving a portion of tissue (including the thin periosteum) adherent to the cortex. Another key instrument is the Orban gingivectomy knife, which safely speeds up the split-thickness dissection at the crest and helps to build a laterally repositioned flap. It must be sharpened by hand.
What if the buccal cortex is too thin and risks fracturing?
The presence of the periosteum and the supracrestal connective tissue is not only a biological matter but also a biomechanical one. This tissue makes the underlying bone wall more elastic, moldable and fracture-resistant. A thin cortex with its periosteum preserved is more likely to flex without fracturing than a denuded cortex of the same size. If the cortex is extremely thin (under one millimeter), consider alternative approaches such as progressive expansion techniques, or reconsider whether the split crest is really the right indication for that specific case.
How long does the split gap take to fully ossify?
The gap fills with a clot that turns into osteoid tissue at a rate of about 1 micrometer per day. The osteoid mineralizes in about ten days, becoming woven bone. This fast process requires the mobilized buccal cortex to stay vital and vascularized. Staffileno’s histologic studies show that with the partial-thickness flap osteogenesis is early, already evident at 14-21 days, with complete restitutio ad integrum at 60 days. With the full-thickness flap, instead, osteogenesis is delayed, starts after 21 days and is still incomplete at 60 days.
How do I manage cases with very dense bone in the mandible?
Dense bone is a greater challenge for the split crest, but the biological principles stay the same. The partial-thickness flap is even more critical because dense cortex has lower intrinsic vascularization and depends more on the periosteal supply. For the osteotomy in dense bone, consider using diamond discs or very-low-speed burs with abundant irrigation. Progression must be even slower and more controlled. Carefully assess whether expansion is truly feasible or whether alternative techniques are indicated.
Is it always mandatory to use the Beaver 64 and 69, or can I improvise?
It’s not the specific instrument that matters but the result you get: a flap that leaves the periosteum and a portion of connective tissue adherent to the bone. The Beaver 64 and 69 are perfect for this and make the work far easier thanks to their round head, which dissects the connective layers without perforating. You can technically get the same result with other instruments, but it takes more skill and increases the risk of errors. A partial-thickness flap made with a 15c blade (as seen in some studies) is an oxymoron. If you don’t have access to these specific instruments, invest in acquiring them before attempting the technique. Saving on an instrument does not justify the risk of compromising the clinical result.
What happens if I’ve already made a full-thickness flap by mistake?
If you notice the mistake during surgery and haven’t made the osteotomy yet, assess whether you can convert to an alternative technique that doesn’t require mobilizing the cortex. If you’ve already mobilized the cortex with a full-thickness flap, the damage is done but you can limit the consequences: use very-low-speed rotary instruments instead of piezo to minimize thermal damage, apply resorbable membranes to protect the mobilized cortex, consider bone substitutes in the gap to mechanically support healing, and inform the patient that the result may be less predictable. In future cases, learn from the mistake and apply the technique correctly.
Want to dig deeper into these topics and stay current with techniques that actually work? Subscribe to the updates at Bonebenders.com and get content that goes beyond congress marketing, into the clinical substance that makes the difference between a result and a failure.
If you’re looking for an oral surgeon experienced in ridge expansion, you can book a consultation.
FAQ
- Why is the partial-thickness flap so important in split crest?
- The periosteum and the supracrestal connective tissue hold the osteoblast progenitor cells and the vascular supply that keeps the outer cortex alive. When you mobilize the buccal cortex with the split, it stays attached to the periosteum and keeps its vitality. The gap fills with a clot that turns into new bone only if the mobilized wall stays alive. Stripping the bone with a full-thickness flap tears away this biological infrastructure. A denuded cortex behaves like a free graft with no vascularization and largely resorbs.
- Can I use piezosurgery for the split crest?
- Piezosurgery can be used, but with extreme caution. Vibrating inserts generate a lot of heat even under abundant irrigation, easily exceeding forty degrees in the areas of greatest friction. In normally vascularized bone the blood flow disperses the heat, but in bone already denuded of its periosteum, with compromised vascularization, that heat becomes lethal for the cells. If you prefer piezo for precision, irrigation must be abundant to the point of being annoying and the progression very slow. Low-speed rotary instruments (100-200 rpm) with good irrigation remain the safest choice.
- Which instruments do I need to make a proper partial-thickness flap?
- The ideal instruments are round-headed blades such as the Beaver 64 and 69. The Beaver 69 is smaller and excellent for periodontal surgery too. The Beaver 64 can also be used for an initial bone incision in very complex cases. These blades separate the connective tissue in the deep layers, leaving a portion of tissue (including the thin periosteum) adherent to the cortex. Another key instrument is the Orban gingivectomy knife, which safely speeds up the split-thickness dissection at the crest and helps to build a laterally repositioned flap. It must be sharpened by hand.
- What if the buccal cortex is too thin and risks fracturing?
- The presence of the periosteum and the supracrestal connective tissue is not only a biological matter but also a biomechanical one. This tissue makes the underlying bone wall more elastic, moldable and fracture-resistant. A thin cortex with its periosteum preserved is more likely to flex without fracturing than a denuded cortex of the same size. If the cortex is extremely thin (under one millimeter), consider alternative approaches such as progressive expansion techniques, or reconsider whether the split crest is really the right indication for that specific case.
- How long does the split gap take to fully ossify?
- The gap fills with a clot that turns into osteoid tissue at a rate of about 1 micrometer per day. The osteoid mineralizes in about ten days, becoming woven bone. This fast process requires the mobilized buccal cortex to stay vital and vascularized. Staffileno's histologic studies show that with the partial-thickness flap osteogenesis is early, already evident at 14-21 days, with complete restitutio ad integrum at 60 days. With the full-thickness flap, instead, osteogenesis is delayed, starts after 21 days and is still incomplete at 60 days.
- How do I manage cases with very dense bone in the mandible?
- Dense bone is a greater challenge for the split crest, but the biological principles stay the same. The partial-thickness flap is even more critical because dense cortex has lower intrinsic vascularization and depends more on the periosteal supply. For the osteotomy in dense bone, consider using diamond discs or very-low-speed burs with abundant irrigation. Progression must be even slower and more controlled. Carefully assess whether expansion is truly feasible or whether alternative techniques are indicated.
- Is it always mandatory to use the Beaver 64 and 69, or can I improvise?
- It's not the specific instrument that matters but the result you get: a flap that leaves the periosteum and a portion of connective tissue adherent to the bone. The Beaver 64 and 69 are perfect for this and make the work far easier thanks to their round head, which dissects the connective layers without perforating. You can technically get the same result with other instruments, but it takes more skill and increases the risk of errors. A partial-thickness flap made with a 15c blade (as seen in some studies) is an oxymoron. If you don't have access to these specific instruments, invest in acquiring them before attempting the technique. Saving on an instrument does not justify the risk of compromising the clinical result.
- What happens if I've already made a full-thickness flap by mistake?
- If you notice the mistake during surgery and haven't made the osteotomy yet, assess whether you can convert to an alternative technique that doesn't require mobilizing the cortex. If you've already mobilized the cortex with a full-thickness flap, the damage is done but you can limit the consequences: use very-low-speed rotary instruments instead of piezo to minimize thermal damage, apply resorbable membranes to protect the mobilized cortex, consider bone substitutes in the gap to mechanically support healing, and inform the patient that the result may be less predictable. In future cases, learn from the mistake and apply the technique correctly.
References
Looking for a specialist?
Rigenerazione Ossea a Frosinone →Il Metodo Bonebenders: espansione osteo-mucosa senza innesti
Need a professional opinion?
Book an appointment at Dr. Bruschi's practice in Frosinone. First visit includes full diagnosis and personalised treatment plan.
Stai valutando un impianto dentale?
Ho scritto una guida in 8 capitoli che spiega tutto quello che un paziente dovrebbe sapere prima di sedersi in poltrona. Niente marketing — solo fatti, casi studio e una checklist per fare le domande giuste.
Scarica la guidaStay Updated
New articles on periodontology, implantology and oral surgery — delivered to your inbox.
Comments
Loading comments...
Leave a comment